SOAPReport-v1.3(2022EN)
General information
Name: nl.zorg.SOAPReport ![]()
Version: 1.3
HCIM Status:Final
Release: 2022
Release status: Prepublished
Release date: 15-10-2023
Metadata
| DCM::CoderList | |
| DCM::ContactInformation.Address | * |
| DCM::ContactInformation.Name | * |
| DCM::ContactInformation.Telecom | * |
| DCM::ContentAuthorList | |
| DCM::CreationDate | 25-5-2020 |
| DCM::DescriptionLanguage | nl |
| DCM::EndorsingAuthority.Address | |
| DCM::EndorsingAuthority.Name | PM |
| DCM::EndorsingAuthority.Telecom | |
| DCM::Id | 2.16.840.1.113883.2.4.3.11.60.40.3.13.6 |
| DCM::KeywordList | Notitie, Verslag, SOEP |
| DCM::LifecycleStatus | Final |
| DCM::ModelerList | Zib centrum |
| DCM::Name | nl.zorg.SOEPVerslag |
| DCM::PublicationDate | 15-10-2023 |
| DCM::PublicationStatus | Prepublished |
| DCM::ReviewerList | |
| DCM::RevisionDate | 05-09-2023 |
| DCM::Supersedes | nl.zorg.SOEPVerslag-v1.2 |
| DCM::Version | 1.3 |
| HCIM::PublicationLanguage | EN |
Revision History
Only available in Dutch
Publicatieversie 1.0 (01-09-2020)
Publicatieversie 1.1 (01-12-2021)
Issue summaries niet beschikbaarBevat: ZIB-1418, ZIB-1473.
Publicatieversie 1.2 (10-06-2022) Bevat: ZIB-1474.
Publicatieversie 1.3 (15-10-2023) Bevat: ZIB-1841, ZIB-1920.
Concept
A SOAP report is a textual report of (partial) contact of the consultation with regard to one problem according to the SOAP method. SOAP (acronym for subjective, objective, assessment, plan) is a method used by health professionals to structurally record information that comes up during contact between the patient and a health professional in the patient's record.The following standardized format is used for reporting:
- Subjective: the patient's complaint and request for help and the amnesic data.
- Objective: the findings from the physical and supplementary examination.
- Assessment: the working hypothesis and the thinking process, for example a differential diagnosis of the healthcare professional.
- Plan: the diagnostic plan or treatment plan and what has been discussed or agreed with the patient.
Purpose
The structure of a SOAP Report offers a care provider the opportunity to record information in a structured manner in free text about one problem and a (partial) contact with a patient. Due to the standardized method of recording SOAP reports over time, it is also possible to follow the patient's condition and its treatment over time.
The SOAP report is mainly used in general practice care.Information Model
Type Id Concept Card. Definition DefinitionCode Reference 
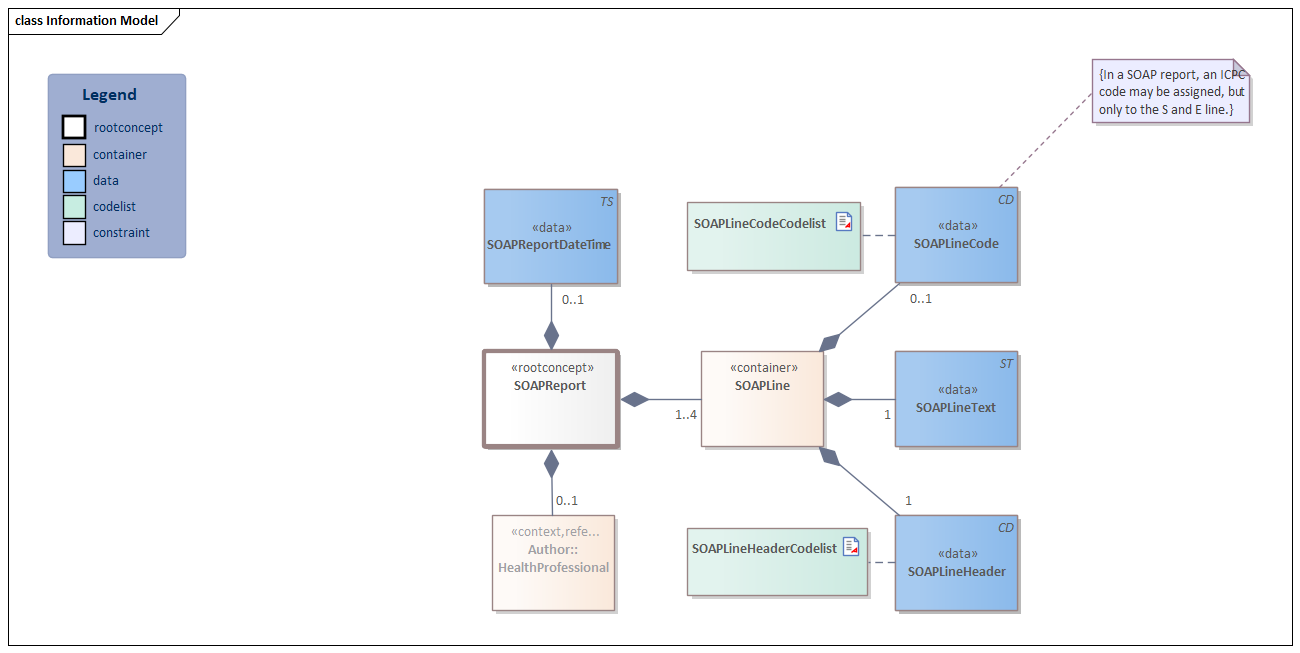
NL-CM:13.6.1  SOAPReport
SOAPReport
Root concept of the SOAPReport information model. This root concept contains all data elements of the SOAPReport information model. 
NL-CM:13.6.2  SOAPReportDateTime
SOAPReportDateTime
0..1 Date and time when the report was recorded. 
NL-CM:13.6.3 Author::HealthProfessional
0..1 The healthcare professional who prepared the report and who is responsible for its content. 
HealthProfessional 
NL-CM:13.6.4 SOAPLine
1..4 Container of the SOAPLine concept. This container contains all data elements of the SOAPLine concept. 
NL-CM:13.6.5 SOAPLineCode
0..1 Coded values can be added to a line that describe essential aspects of the line. In a SOAP report an ICPC code may be assigned, but only to the S and A line.
11591000146107 Patient encounter report 
SOAPLineCodeCodelist
NL-CM:13.6.6 SOAPLineHeader
1 The name of the SOAP line as a coded description. In a SOAP report this can be one of the following: subjective, objective, assessment or plan. SOAPLineHeaderCodelist 
NL-CM:13.6.7 SOAPLineText
1 The actual content of the section as free formatted text. 422813005 Document section Columns Concept and DefinitionCode: hover over the values for more information
For explanation of the symbols, please see the legend page
Example Instances
Only available in Dutch
Voorbeeld file fout: Unable to find the specified file. : nl.zorg.Zib of versie niet gevonden-v1.3(NL)_Voorbeeld.docx
Traceability to other Standards
This health and care information model is based on the information model template ClinicalNote-v1.0.
Valuesets
SOAPLineCodeCodelist
Valueset OID: 2.16.840.1.113883.2.4.3.11.60.40.2.13.6.1 Binding: Required Conceptname Codesystem name Codesystem OID All values ICPC-1 NL 2.16.840.1.113883.2.4.4.31.1 SOAPLineHeaderCodelist
Valueset OID: 2.16.840.1.113883.2.4.3.11.60.40.2.13.6.2 Binding: Required Conceptname Conceptcode Codesystem name Codesystem OID Description Subjective 255362007 SNOMED CT 2.16.840.1.113883.6.96 Subjectief, (S) Objective 260224007 SNOMED CT 2.16.840.1.113883.6.96 Objectief, (O) Evaluation - action 129265001 SNOMED CT 2.16.840.1.113883.6.96 Evaluatie, (E) Management - action 129271007 SNOMED CT 2.16.840.1.113883.6.96 Plan, (P) This information model in other releases
- Release 2020, (Version 1.0)
- Prerelease 2021-2, (Version 1.1)
- Prerelease 2023-1, (Version 1.3)
- Release 2024, (Version 1.3.1)
- Prerelease 2026-1, (Version 1.3.1)
Information model references
This information model refers to
This information model is used in
- --
Technical specifications in HL7v3 CDA and HL7 FHIR
To exchange information based on health and care information models, additional, more technical specifications are required.<BR> Not every environment can handle the same technical specifications. For this reason, there are several types of technical specifications:
- HL7® version 3 CDA compatible specifications, available through the Nictiz ART-DECOR® environment

- HL7® FHIR® compatible specifications, available through the Nictiz environment on the Simplifier FHIR

Downloads
This information model is also available as pdf file
 or as spreadsheet
or as spreadsheet 
About this information
The information in this wikipage is based on Pre-release 2022-1
SNOMED CT and LOINC codes are based on:- SNOMED Clinical Terms versie: 20230930 [R] (september 2023-editie)
- LOINC version 2.76
Conditions for use are located on the mainpage
This page is generated on 27/03/2024 09:34:27 with ZibExtraction v. 9.3.8851.20230